|
Overview
 Bunions are bony bumps that form on the side of the big toe joint or baby toe joint (these are commonly called ?bunionettes? or ?tailor?s bunions?). Bunions most commonly result from one or more of the following factors: genetics, faulty foot mechanics like over-pronation, and/or long periods of time spent in improperly fitting footwear. Bunions can start with audible clicking (called ?crepitus?) and/or stiffness in the affected joint which indicates that the joint surfaces are rubbing together improperly. This may progress to include inflammation, degeneration of the surfaces of the joint, deformity (including bone growth at the joint line and displacement of the toe) and ultimately, loss of range of motion in the joint. Bunions are bony bumps that form on the side of the big toe joint or baby toe joint (these are commonly called ?bunionettes? or ?tailor?s bunions?). Bunions most commonly result from one or more of the following factors: genetics, faulty foot mechanics like over-pronation, and/or long periods of time spent in improperly fitting footwear. Bunions can start with audible clicking (called ?crepitus?) and/or stiffness in the affected joint which indicates that the joint surfaces are rubbing together improperly. This may progress to include inflammation, degeneration of the surfaces of the joint, deformity (including bone growth at the joint line and displacement of the toe) and ultimately, loss of range of motion in the joint.Causes Many problems that occur in the feet are the result of abnormal pressure or rubbing. One way of understanding what happens in the foot due to abnormal pressure is to view the foot simply. Our simple model of a foot is made up of hard bone covered by soft tissue that we then put a shoe on top of. Most of the symptoms that develop over time are because the skin and soft tissue are caught between the hard bone on the inside and the hard shoe on the outside. Any prominence, or bump, in the bone will make the situation even worse over the bump. Skin responds to constant rubbing and pressure by forming a callus. The soft tissues underneath the skin respond to the constant pressure and rubbing by growing thicker. Both the thick callus and the thick soft tissues under the callus are irritated and painful. The answer to decreasing the pain is to remove the pressure. The pressure can be reduced from the outside by changing the pressure from the shoes. The pressure can be reduced from the inside by surgically removing any bony prominence. Symptoms Look for an angular, bony bump on the side of the foot at the base of the big toe. Sometimes hardened skin or a callus covers this bump. There's often swelling, redness, unusual tenderness, or pain at the base of the big toe and in the ball of the foot. Eventually, the area becomes shiny and warm to the touch. Seek medical advice if you have persistent pain when walking normally in otherwise comfortable, flat-soled shoes, you may be developing a bunion, bursitis, or a bone spur in your foot. Diagnosis Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly. Non Surgical Treatment Bunions may be treated with proper shoes and corrective inserts such as toe spacers, bunion or toe separators, as well as bunion cushions and splints. In extreme cases, surgery may be needed to remove the bony enlargement of the first metatarsal bone, realigning the bone, or straightening the big toe.  Surgical Treatment Many studies have found that 85 to 90 percent of patients who undergo bunion surgery are satisfied with the results. Fewer than 10 percent of patients experience complications from bunion surgery. Possible complications can include infection, recurrence of the bunion, nerve damage, and continued pain. If complications occur, they are treatable but may affect the extent of your full recovery. Prevention Because bunions develop slowly, taking care of your feet during childhood and early adulthood can pay off later in life. Keep track of the shape of your feet as they develop over time, especially if foot problems run in your family. Exercising your feet can strengthen them. Learn to pick up small objects, like a pencil or pebble, with your toes. Wear shoes that fit properly and don't cramp or pinch your toes. Women should avoid shoes with very high heels or pointed toes. Overview
Excessive pronation hampers our natural walking pattern, causing an imbalance and leading to wear and tear in other parts of the body, with every step we take! Whether you have a true flat foot or suffer from over-pronation in both cases your poor walking pattern may contribute to a range of different complaints. Especially with age, poor alignment of the feet will cause very common conditions such as heel pain or knee Pain.  Causes Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch. Symptoms Symptoms can manifest in many different ways. The associated conditions depend on the individual lifestyle of each patient. Here is a list of some of the conditions associated with over Pronation. Hallux Abducto Valgus (bunions). Hallux Rigidus (stiff 1st toe). Arch Pain. Heel Pain (plantar Facsitus). Metatarsalgia (ball of the foot pain). Ankle Sprains. Shin Splints. Achilles Tendonitis. Osteochondrosis. Knee Pain. Corns & Calluses. Flat Feet. Hammer Toes. Diagnosis A quick way to see if you over-pronate is to look for these signs. While standing straight with bare feet on the floor, look so see if the inside of your arch or sole touches the floor. Take a look at your hiking or running shoes; look for wear on the inside of the sole. Wet your feet and walk on a surface that will show the foot mark. If you have a neutral foot you should see your heel connected to the ball of your foot by a mark roughly half of width of your sole. If you over-pronate you will see greater than half and up to the full width of your sole.  Non Surgical Treatment Podiatrists are trained to effectively detect and management over-pronation. You can get a referral to a podiatrist from your GP if you are presenting with the pain typical of over-pronation, or you can seek private podiatric care in anyone of several registered and accredited practices across the country. Your podiatrist will examine your foot and its shape to determine whether or not over-pronation is the cause of your pain. If your podiatrist determines that it is a problem with arch support that is giving you trouble, then they can effectively remedy that lack of support with orthotics. Surgical Treatment Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint. Overview
Foot pain is not only limited to grown-ups. Often, healthy and active children will complain of pain in one or both heels shortly after running, engaging in sports or even walking. The pain is centered at the back of, or under the heel. The cause of heel pain in children is usually a condition called calcaneal apophysitis, normally reported by 8 to 14 year olds. Causes One of the most common causes of heel pain in adolescents, Sever's disease is an overuse injury to the growth plate of the calcaneus (heel). It is commonly seen in growing, active children 8-12 years of age. Soccer players, gymnasts, and children who do any sort of running or jumping activity have an increased risk of developing Sever's disease. Occurring in one or both feet, Sever?s disease occurs at the back of the heel (also known as the apophysis or the insertion of the Achilles tendon). Symptoms Sever's disease causes pain and tenderness in the back and bottom of the heel when walking or standing, and the heel is painful when touched. It can occur in one or both feet. Diagnosis Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture. Non Surgical Treatment Sever?s disease treatment should be based on eliminating pain and restoring normal foot and leg biomechanics. As with most soft tissue injuries the initial treatment is Rest, Ice, and Protect. In the early phase you?ll most likely be unable to walk pain-free. Our first aim is to provide you with some active rest from pain-provoking activities. "No Pain. No Gain." does not apply in Sever's disease. If it hurts your child is doing too much exercise. Your child should reduce or cease any activity that causes heel pain. Ice is a simple and effective modality to reduce your pain and swelling. Please apply for 20-30 minutes each 2 to 4 hours during the initial phase or when you notice that your injury is warm or hot. Most children can tolerate paracetamol as a pain reducing medication. Check with your doctor. To support and protect your heels, you may need to be wear shock absorbing heel cups or a soft orthotic. Kinesio foot taping may help to provide pain relief. Your physiotherapist will guide you and utilise a range of pain relieving techniques including joint mobilisations for stiff ankle or subtalar joints, massage or electrotherapy to assist you during this pain-full phase. Overview
Plantar fasciitis is a common and often persistent kind of repetitive strain injury afflicting runners, walkers and hikers, and nearly anyone who stands for a living, cashiers, for instance. It causes mainly foot arch pain and/or heel pain. Morning foot pain is a signature symptom. Plantar fasciitis is not the same thing as heel spurs and flat feet, but they are related and often confused. Most people recover from plantar fasciitis with a little rest, arch support (regular shoe inserts or just comfy shoes), and stretching, but not everyone. Severe cases can stop you in your tracks, undermine your fitness and general health, and drag on for years.  Causes There are several reasons why arch pain develops. Sometimes it?s due to a condition known as plantar fasciitis, in which the plantar fascia (the band of tissue that runs along the bottom of your foot from your heel to your toes) becomes inflamed after excessive stress. Heel pain results from this inflammation. Sometimes the pain is due to extensive time spent on your feet. Many people feel pain on the arch of their feet after a long workday, while others overuse their feet exercising or playing sports. A foot deformity, such as hammertoe or clubfoot, can also cause this pain. Medical conditions such as diabetes or obesity can put additional stress on your feet, thereby causing arch pain. Your footwear is also important. Shoes should support all parts of your foot, especially the bottom. This is very important if you spend excessive time on your feet, if your obese, if your pregnant, or if you engage in sport-related activities. Injuries to any of the twenty-six bones, thirty-three joints and over 100 muscles, tendons and ligaments in the feet can also cause arch pain. Because the foot is such a complex structure, it?s important to see a podiatrist at the first sign of symptoms. Symptoms Flat feet can exhibit a variety of symptoms, from mild to severe. The extent of the flat foto does not always correlate with the extent of symptoms. Patients may complain of arch pain and heel pain. Commonly there is pain on the outside of the foot, where the foot meets the ankle as the collapse foot abuts against the ankle. Muscle cramps within the foot, and onto the leg (shin splints) may occur. In general, patients have pain with activity, such as walking or running. The pain may be deep and focal to a generalized widespread achy feeling. Irritation from shoe gear can cause redness and swelling. Common reasons patients seek treatment are pain, interference with walking or activities, difficulty fitting shoes, swelling, and notice a change in appearance of the foot and/or unsightly appearance. Diagnosis The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma. Non Surgical Treatment If you have arch pain, you need proper arch support. You can get arch support by purchasing custom shoe inserts that are made to support your feet. If you have flat feet or high arches, you can certainly benefit from arch support inserts. Take a look at your wet footprint; if you notice that your footprint is completely filled in, then you have flat feet. On the other hand, if there is a large crescent shape missing from your footprint, then you have high arches. Both of these conditions require proper support from a shoe insert. Foot Solutions You can also take care of your feet by avoiding high heels and flip-flops. If you must wear high heels, choose a heel that is two inches or less, and try to wear them only for short periods of time. Flip-flops provide very little support, so wear them only if you won?t be doing very much walking.  Surgical Treatment The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot. Prevention Because most cases of flatfeet are inherited, the condition is usually impossible to prevent. Even when children with flexible flatfeet are treated with arch supports and corrective shoes, there is little evidence that these devices prevent the condition from lasting into adulthood.
Overview
 The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon. The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon.Causes Common causes of an Achilles tendon rupture include the progression of or the final result of longstanding Achilles tendonitis or an overuse injury. An injury to the ankle or a direct blow to the Achilles tendon. As a result of a fall where an individual lands awkwardly or directly on the ankle. Laceration of the tendon. Weakness of the gastrocnemius or soleus muscles in people with existing Achilles tendonitis places increased stress on the tendon. Steroid use has been linked to tendon weakness. Certain systemic diseases have been associated with tendon weakness. A sudden deceleration or stopping motions that cause an acute traumatic injury of the ankle. Injection of steroids to the involved tendon or the excessive use of steroids has been known to weaken tendons and make them susceptible to rupture. Contraction of the calf muscles while the foot is dorsiflexed (pointed toward the head) and the lower leg is moving forward. Symptoms Patients who suffer an acute rupture of the Achilles tendon often report hearing a "pop" or "snap." Patients usually have severe pain the back of the lower leg near the heel. This may or may not be accompanied by swelling. Additionally, because the function of the Achilles tendon is to enable plantarflexion (bending the foot downward), patients often have difficulty walking or standing up on their toes. Diagnosis Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed. Non Surgical Treatment The most widely used method of non-surgical treatment involves the use of serial casting with gradual progression from plantar flexion to neutral or using a solid removable boot with heel inserts to bring the ends of the tendon closer together. The advantage of a solid removable boot is that it allows the patient to begin early motion and is removable. Wide variability exists among surgeons in regards to the period of absolute immobilization, initiating range of motion exercises, and progression of weight bearing status. 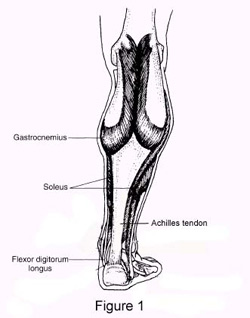 Surgical Treatment There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down. |
